What is Acromegaly?

Acromegaly is a rare hormonal disorder characterized by excessive secretion of growth hormone after the completion of body growth. The primary trigger for acromegaly is often a benign tumor (known as an adenoma) in the pituitary gland, which results in an overproduction of growth hormone. This surplus growth hormone leads to a variety of symptoms, such as larger hands and feet, oily skin, and increased perspiration.
Overproduction of growth hormone prompts the liver to manufacture insulin-like growth factor 1 (IGF-1). This is another type of hormone that plays a crucial role in the development of acromegaly.
In a person with this disorder, the excess production of growth hormone causes a rise in IGF-1 levels in the bloodstream. This increase can contribute to the distinct symptoms of the disorder, including enlargement of the hands and facial features.
Given the importance of our hands and feet in everyday life, even a seemingly simple act like wearing an engagement ring can pose difficulties for those living with acromegaly. The following is an introduction to this rare disorder, with an overview of symptoms, causes, and diagnosis.
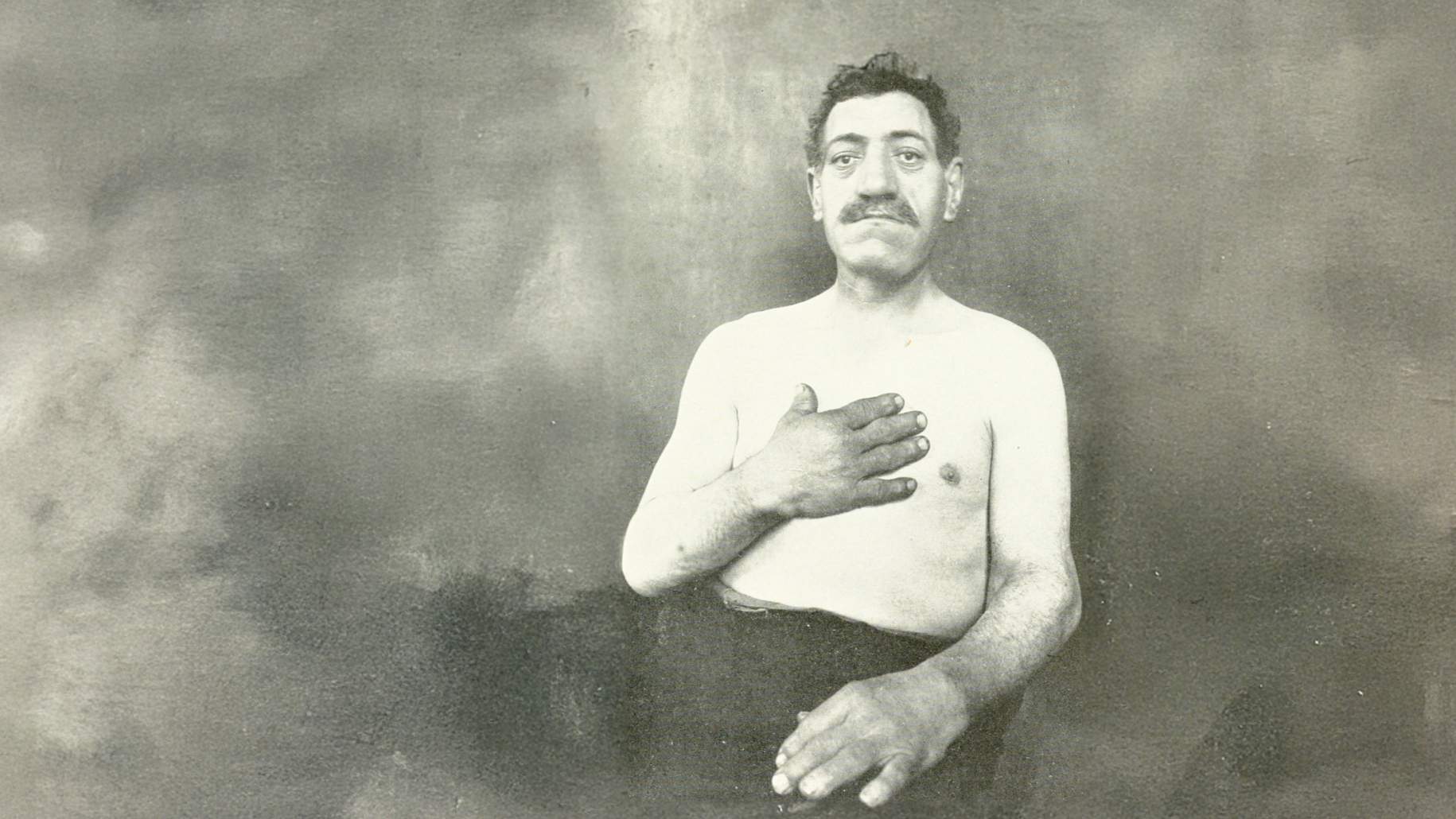
What Are the Symptoms?
Symptoms associated with acromegaly can greatly differ among individual patients. For instance, only approximately 1 in 4 (roughly 25%) patients with acromegaly have high blood pressure.
However, an estimated 95% of patients typically experience an enlargement of their hands and feet. The following are some potential symptoms and characteristics of acromegaly:
- Enlarged hands and feet
- Protruding jaw, enlarged nose, and spaced-out teeth
- Headaches
- Sweaty and oily skin
- Deepened voice
- Muscle fatigue and joint pain
- Sleep apnea
- Carpal tunnel syndrome
- Abnormal menstrual cycles (in women)
How Common Is Acromegaly?
Acromegaly can affect anyone regardless of their age, sex, ethnic background, or geographic location, but it is relatively uncommon in contrast to other hormonal disorders. Although acromegaly typically starts in adulthood, between the ages of 30 and 50 years, it can appear at any age.
The disorder's prevalence is the same across diverse populations and ethnicities, with no apparent inclination toward any particular group. It occurs in approximately 40 to 125 per 1 million (0.004%–0.013%) of people.
Unfortunately, there is no known prevention for acromegaly, but early treatment can prevent the disease from getting worse and help avoid complications.
Why should you have your surgery with Dr. Cohen?
Dr. Cohen
- 7,500+ specialized surgeries performed by your chosen surgeon
- More personalized care
- Extensive experience = higher success rate and quicker recovery times
Major Health Centers
- No control over choosing the surgeon caring for you
- One-size-fits-all care
- Less specialization
For more reasons, please click here.
How Is Acromegaly Diagnosed?
The diagnosis of acromegaly typically involves a review of the patient’s medical history, a physical examination, and laboratory testing. Common laboratory tests include IGF-1 measurement and the oral glucose tolerance test. These 2 tests are widely recognized as the gold-standard assessments for diagnosing the disease.
- IGF-1 testing—evaluates the level of IGF-1 in the blood. This hormone is generated by the liver in response to the presence of growth hormone. In those with acromegaly, the IGF-1 level is often high, which makes this test a standard diagnostic procedure.
- Oral glucose tolerance test—often used to validate the diagnosis of acromegaly. During this test, the patient ingests a solution that contains a specified amount of glucose, and blood samples are collected at set intervals to monitor growth hormone levels. In people not affected by acromegaly, the growth hormone level typically drops after glucose consumption. However, in those with the disorder, the levels remain persistently high.
- Imaging tests—Imaging tests, including magnetic resonance imaging (MRI) and computed tomography (CT) are utilized to assess the size, shape, location, and characteristics of the causative tumor. If no tumor is found in the brain or pituitary gland, your care team may obtain additional tests of your chest, abdomen, or pelvis in order to locate the culprit lesion.
What Are the Causes?
The primary cause of acromegaly is usually a benign tumor, known as an adenoma, in the pituitary gland. This tumor triggers the gland to secrete an excessive quantity of growth hormone, which leads to unusual growth of bones and tissues throughout the body.
In addition, the tumor can exert pressure on different parts of the brain, resulting in symptoms such as visual headaches and other neurological deficits. In more than 90% of people with acromegaly, the overproduction of growth hormone originates from this benign pituitary tumor.
In less common instances, a tumor situated in a place other than the pituitary gland, such as the pancreas, lungs, or adrenal glands, can result in the overproduction of growth hormone–releasing hormone, which prompts the pituitary gland to generate an excess of growth hormone.
Because it refers to a specific condition characterized by the overproduction of growth hormone in adults, acromegaly does not have different “types.” However, there can be variations in the underlying cause of acromegaly, and these variations can affect how the disorder is managed and treated.
Key Takeaways
- Four features of acromegaly include excessive growth of the hands and feet, enlarged facial features, thickened skin, and joint pain
- The primary cause is usually a benign tumor (called an adenoma) in the pituitary gland
- The estimated incidence is approximately 40 to 125 cases per 1 million people
- Common laboratory tests for acromegaly include IGF-1 measurement and an oral glucose tolerance test











