High-Grade Glioma

Written by: Aaron Cohen-Gadol, MD
Last Updated: October 4, 2024
See our Medical Editorial Standards for more information about how we maintain the highest standards of medical accuracy.
Gliomas are tumors of the central nervous system, which is made up of the brain and spinal cord. These tumors are more often seen in the brain than in the spinal cord. Gliomas are classified by their rate of growth and invasion of other tissues (grade). Grades I and II are considered low-grade, while Grades III and IV are considered high-grade. Grade IV is the most aggressive, being the fastest growing and most invasive.
What Causes High-Grade Glioma?
High-grade gliomas commonly develop from lower grade gliomas; however, they also can occur spontaneously. Gliomas are caused by changes, or mutations, in the glial cell DNA. The exact mechanism of these changes remains to be discovered, although some risk factors are known.
Gliomas have been associated with exposure to certain types of radiation. Microwave ovens and power lines have not conclusively shown any association. Certain toxins have also been implicated. Advanced age, white race, male gender, and family history of glioma can also increase risk.
Signs and Symptoms of High-Grade Glioma
High-grade and low-grade gliomas have the potential to cause the same symptoms; however, symptoms arising from high-grade gliomas may be more pronounced, noticeable, or progressive. When gliomas affect the brain, they can cause:
- Headaches
- Seizures, or increase in seizures in patients with seizure disorders
- Nausea and vomiting
- Difficulty thinking or remembering
- Irritability or other personality changes
- Problems with balance
- Urinary incontinence
- Difficulty speaking
Why should you have your surgery with Dr. Cohen?
Dr. Cohen
- 7,000+ specialized surgeries performed by your chosen surgeon
- More personalized care
- Extensive experience = higher success rate and quicker recovery times
Major Health Centers
- No control over choosing the surgeon caring for you
- One-size-fits-all care
- Less specialization
For more reasons, please click here.
How Are Gliomas Diagnosed?
As in many fields of medicine, the first step in diagnosis is a thorough history and physical examination. At your visit, the physician will ask you several questions about your signs and symptoms, possible exposures, and family history. Next he or she will perform a physical examination, with an emphasis on neurological function.
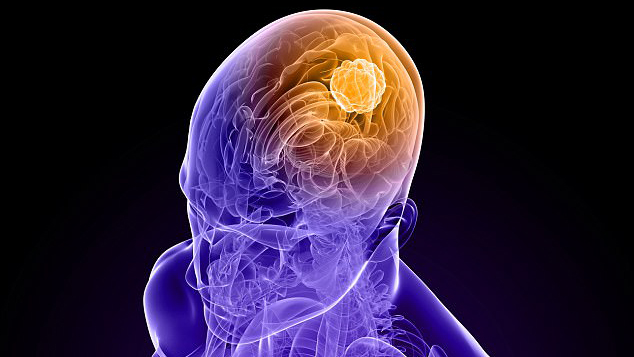
If your doctor suspects a tumor of the nervous system, he or she may order a combination of blood work, computed tomography (CT) scan, magnetic resonance imaging (MRI), and other pertinent tests.

Figure 1: This MRI demonstrates a high-grade glioma in the left temporal and frontal lobes.
If a tumor is found, you will be referred to a neurosurgeon who will then determine the type and nature of the tumor through a biopsy (stereotactic biopsy) or resection (removal) of the tumor via surgery to open the skull bone known as a craniotomy. A biopsy procedure involves removal of a small part of the tumor for diagnosis only. The biopsy specimen is sent to the pathology lab, where another physician, called a pathologist, will examine it under a microscope. After the character of the tumor is known, you and your doctor can establish a treatment strategy. During a craniotomy for resection, the neurosurgeon attempts to remove most of the tumor safely.
Treatment of High-Grade Glioma
Many factors influence treatment strategies for high-grade gliomas. Surgery is a common method of treatment and has been shown to improve outcomes in certain cases. Radiation and chemotherapy can be used alone or in addition to surgery. Radiation can prevent the tumor from growing and, in some cases, actually shrink certain tumors. Focused beams of radiation are aimed at the tumor for a short duration of time (5 to 15 minutes) over the course of several visits. Chemotherapy may be oral or intravenous and provides another method for reducing tumor growth.
Temodar (temozolomide) may be given before radiation therapy to sensitize the tumor to radiation. It is often taken by mouth once a day. Your doctor may prescribe other medications along with it, to prevent nausea. Avastin (bevacizumab) is often given intravenously every two weeks. It works by preventing growth of new blood vessels that the tumor attempts to produce as it invades healthy tissue.
What Is the Prognosis of High-Grade Glioma?
Survival outcomes and prognoses of patients with high-grade gliomas are variable and can depend upon several factors. Patients with high-grade oligodendrogliomas and certain astrocytomas can live for years, while patients with glioblastoma may have dramatically shorter life expectancies. It is unfortunately not uncommon for patients with glioblastoma to survive for ten months or less. Each patient’s case is unique, and overgeneralization should be avoided. The treatment plan and prognosis for your individual case should be discussed with your neurosurgeon. Please seek experienced surgeons and multidisciplinary teams to assure effective therapies.